It is now well known that ongoing tobacco use is associated with poorer survival in people with lung cancer. The IASLC Board formed the Tobacco Control & Smoking Cessation Committee in 2012 in order to provide advice and direction to activities and initiatives that the Association should engage in to reduce the use of tobacco worldwide. The Committee ensures that IASLC addresses the needs of practitioners seeking to help their patients stop tobacco use. This Committee will recommend actions to contribute to international, national, and local efforts in tobacco control research, initiatives, and interventions.

Committee projects
Chair of Committee

Mahdi Sheikh
2025-2027
2025-2027 Roster

Joelle Fathi
United States
University of Washington
Committee Member

Stephanie Land
United States
National Cancer Institute
Committee Member

Matthew Steliga
United States
University of Arkansas
Committee Member
Committee Responsibilities:
- Develop and implement programs to educate IASLC members on the most effective methods to assist their patients to stop tobacco use, particularly smoking, in order to improve tobacco treatment outcomes and survival and to prevent second malignancies.
- Develop and implement recommendations to disseminate information to IASLC members and other healthcare providers through education and publication activities.
- Inventory current IASLC programs and recommend support for studies in lung cancer patients or implementation of studies or programs involving tobacco cessation.
- Develop relationships with local, national, and international organizations supporting similar initiatives and identify opportunities for collaboration.
- Make recommendations as needed to ensure that the IASLC Statement on Tobacco is comprehensive and up to date.
- Make recommendations on the ways IASLC can support activities to limit the use of trade agreements or other policy mechanisms that promote tobacco use.
- Make recommendations on all strategies that IASLC could support that would reduce tobacco consumption and the use of cigarette additives.
Related Resources


Tobacco Cessation Position Statement Endorsements

National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology – Smoking Cessation
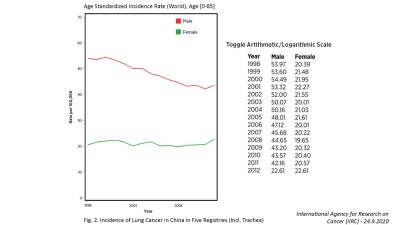
Tobacco smoking has been implicated in causing cancers of the lungs, mouth, lips, nose, sinuses, larynx, pharynx, esophagus, stomach, pancreas, kidney, bladder, uterus, cervix, colon/rectum, ovary, and myeloid leukemia.1 Cancers linked to tobacco use comprise 40% of all cancer diagnoses, and cigarette smoking is linked to 30% of all cancer-related deaths nationwide.2 State-level data suggest that cigarette smoking is responsible for as high as 40% of cancer-related deaths in some geographic regions.3 Lung cancer is the leading cause of cancer-related death in both males and females.4 The recommendations in these guidelines apply to the cessation of cigarette smoking, which poses the greatest risk to patients with cancer. Regardless of stage or treatment modalities, all patients should be encouraged to achieve and maintain abstinence from all combustible tobacco products (e.g., cigarettes, cigars, hookah) and smokeless tobacco products. Smoking cessation has health benefits even after a cancer diagnosis, regardless of site, stage, or prognosis—namely, improvement in cancer treatment outcomes, primary cancer recurrence, and secondary cancers. Importantly, a diagnosis of cancer may present a teachable moment and valuable opportunity for providers to encourage smoking cessation.5-8 It is the view of the NCCN Smoking Cessation Panel that it is never too late for patients with cancer at any stage to stop smoking cigarettes and experience health benefits.
References
- 1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019;69:7–34.30620402
- 2. CDC Vital Signs: Cancer and tobacco use. Accessed January 12, 2023. Available at: https://www.cdc.gov/vitalsigns/pdf/2016-11-vitalsigns.pdf
- 3. Goding SauerA, SiegelRL, et al.State-level cancer mortality attributable to cigarette smoking in the United States. /JAMA Intern Med/2016;176:1792–1798
- 4. SiegelRL, MillerKD, FuchsHE, et al.Cancer statistics, 2022. /CA Cancer J Clin/2022;72:7–33
- 5-8. CarrollAJ, Veluz-WilkinsAK, BlazekovicS, et al.Cancer-related disease factors and smoking cessation treatment: analysis of an ongoing clinical trial. /Psychooncology/2018;27:471–476. GritzER, FingeretMC, VidrineDJ, et al.Successes and failures of the teachable moment: smoking cessation in cancer patients. /Cancer/2006;106:17–27 WestmaasJL, NewtonCC, StevensVL, et al.Does a recent cancer diagnosis predict smoking cessation? An analysis from a large prospective US cohort. /J Clin Oncol/2015;33:1647–1652. TangMW, OakleyR, DaleC, et al.A surgeon led smoking cessation intervention in a head and neck cancer centre. /BMC Health Serv Res/2014;14:636
Related Content